

Possible Pediatric Pathogens
Possible Pediatric Pathogens
What can In-Hospital PCR Detections in children tell us?

As an observer of epidemiological data over the last 2 years of the pandemic, the concept of viral trends and epidemic patterns have become fascinating. The seasonal waves1, regional patterns2, and viral competition3 is incredible when you think about it. Simple trend analysis and observing the patterns of how viruses surge and wane at different times can give us indications of what’s happening in our microbiome.
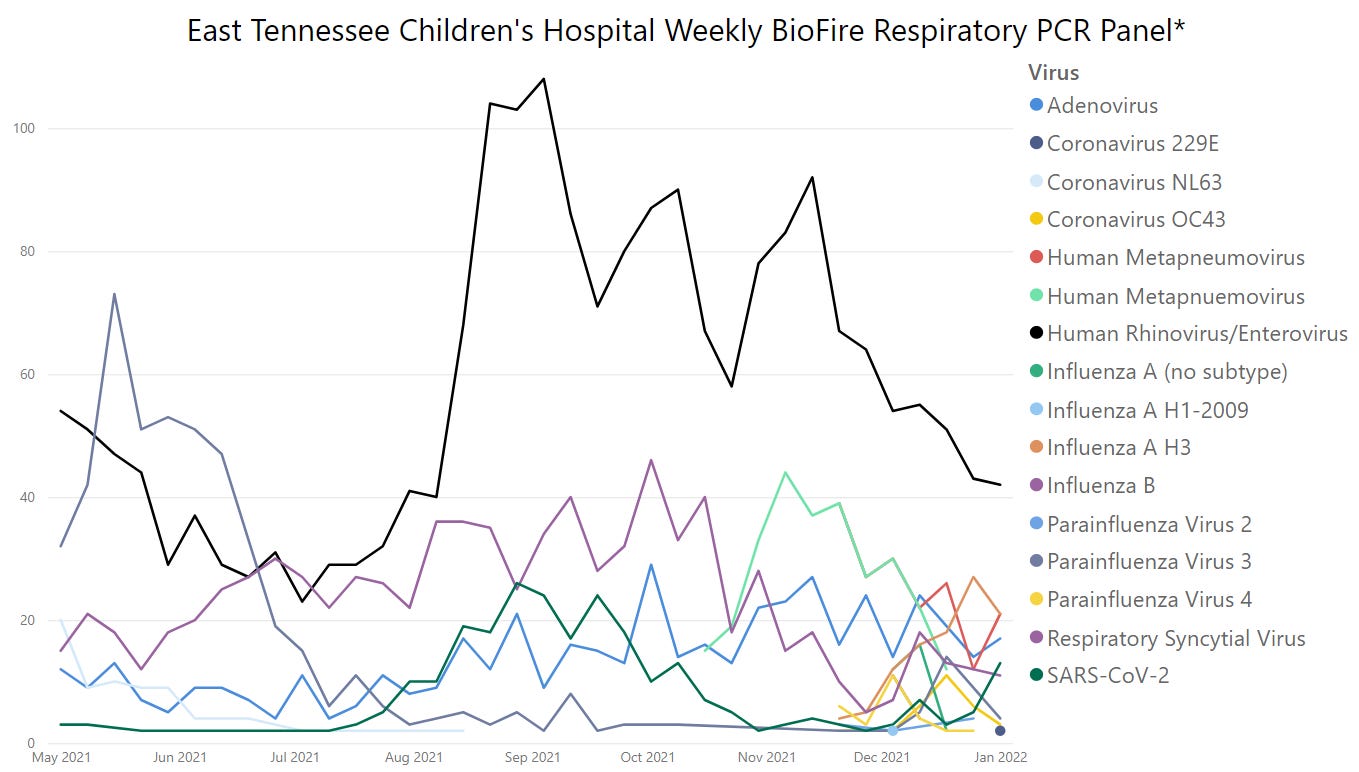
A fascinating phenomenon occurred during the first year of the SARS-COV2 pandemic: other ubiquitous, seasonal4 pathogens all but disappeared from circulation. This was covered well in this piece. Observing the viral trends from BioFire from summer 2020 till now, you can see that throughout 2020 the only 2 circulating pathogens were Rhinovirus and SARS-COV2, till about the summer of 2021.

Typically, winter is known for flu season, as well as RSV and other respiratory illnesses. In summer 2021 this expected pattern was altered when there was a large, unexpected RSV epidemic in the South5 (see purple trend line above). Since RSV season in winter 2020 had been “skipped,” some called this a catch up season. This was not just a US phenomena either, as it occurred globally. One of my favorite Twitter accounts- Viral Myalgia, has a insightful thread on the interesting “co-epidemic” of RSV + SARS-COV2 that occurred in summer 2021.
Like every other aspect of the pandemic, the effects of SARS-COV2 on kids has lacked context and perspective due to the politicization and media driven hysteria. While RSV was surging in summer 2021, there were many who jumped aboard to “Covid is coming after the kids” panic train to take advantage of the increase in illness in kids that very well could have been caused by an entirely different pathogen. This is not to diminish the Delta wave that was certainly real and sent many adults to the hospital and vulnerable kids as well.
Here’s a perfect example from NBC news last summer, where they intentionally bury the fact that RSV was in fact a large part of the reason why kids were seeking medical care.

Down in the article you read “Combined with the rise in out-of-season virus infections this summer…”
RSV can be a particularly nasty bug to kids, specifically children under 5. Currently there’s no widespread vaccine available for RSV. I remember when my own daughter was 7 weeks old, she had a fever that would not break, and we ended up at Vanderbilt children’s hospital a week after Christmas. Like any parent with a first child, taking your child to the hospital is frightening and your mind is racing wondering what could be wrong. When we arrived, we were told they were testing Flu, RSV, and a urinary tract infection. When tests were completed were were told that all three were negative. Her diagnosis: “a virus.” They never even bothered to tell us which one. Why? After giving fluids, getting her temperature down, we were sent home.
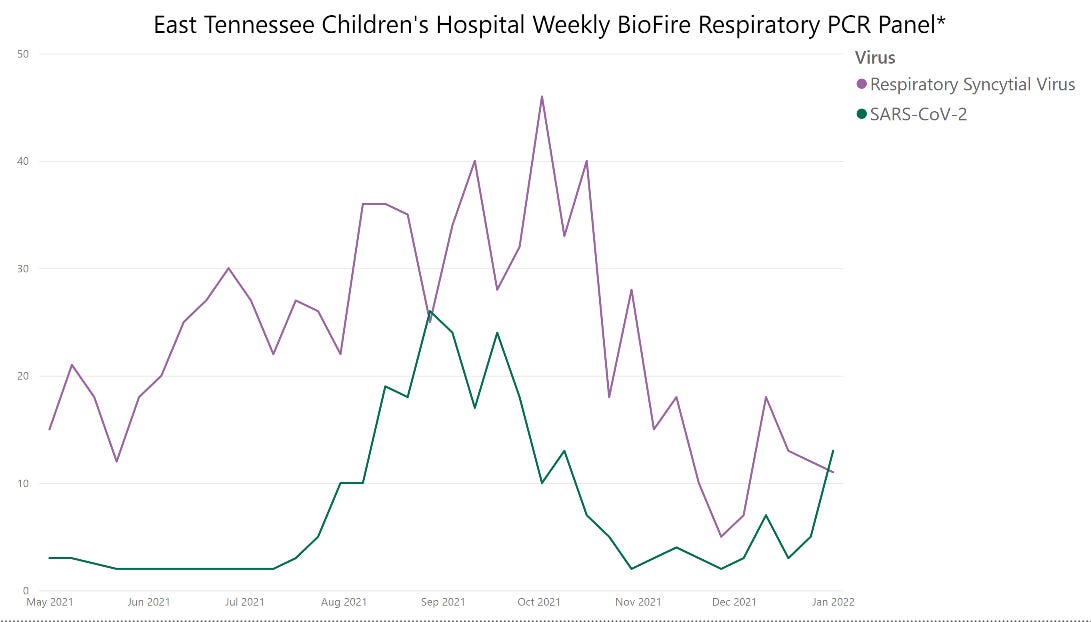
So let’s take a look at the impact of RSV vs. SARS-COV2 last summer. Below is a chart comparing the weekly detections of respiratory pathogens in hospitalized children at East Tennessee Children’s Hospital. This data cannot tell us the reason for a child’s admission to the hospital, however it shows the comparative prevalence of one pathogen vs. the other among hospitalized kids. This is a critical point. For all of the possible pediatric pathogens, which one is the primary culprit that requires hospitalization and treatment? It turns out this really isn’t as straightforward as we would like to think.
One recent paper6 found
“children under 24 months of age hospitalized with respiratory compromise due to COVID-19 were retrospectively analyzed according to the event of coinfection with respiratory syncytial virus. Of 32 patients, 18.7% had coinfection and these had a significantly longer length of stay.”
An NIH Notice of Special Interest (NOSI)7 confirms that co-infection among children is under studied:
“… an unseasonal increase in RSV infections has been reported, with a documented surge in infections in the summer months from May 2021 that is significantly increased compared to previous years. Co-infection with respiratory viruses, particularly RSV with SARS-CoV-2 is resulting, in preliminary surveys, in severe respiratory disease in children and young adults, with a few reports of evidence of chronic ongoing lung damage in babies.”
When we look at pediatric SARS-COV2 hospitalization data, are we getting the full story? Clearly as community rates increase, so do hospitalization detections in both adults and children. But do the ever-present case counts and hospitalization trends really mean what they imply? Journalist David Zweig, easily the bravest and most rigorous journalist throughout the pandemic, has an excellent article on this subject and it gets at the “with vs. from” issue.
Because we are screening every hospital admission for SARS-COV2 for infection control purposes, we are catching cases that might not actually be the reason for their healthcare treatment seeking behavior. Here’s a couple papers8 from the Journal ‘Hospital Pediatrics” that quantified this issue.
“A total of 53 (45%) admissions were categorized as unlikely to be caused by SARS-CoV-2”
“Although COVID-19 has considerable associated morbidity and mortality in children, reported hospitalization rates likely lead to overestimation of the true disease burden.”
“Pediatric patients9 hospitalized with SARS-CoV-2 fall into distinct categories, which are critical to understanding the true pathology of SARS-Cov-2 as it relates to hospitalized pediatric patients. Most hospitalized patients who test positive for SARS-CoV-2 are asymptomatic or have a reason for hospitalization other than coronavirus disease 2019.”
What about Omicron? Dr. Jeanne Noble gets into this issue and discusses incidental hospitalizations with this incredible interview with Dr. Vinay Prasad.
No parent wants their kids to get sick. I’ve been there, and I would never want to diminish the serious and concerning nature of the cases within kids that are severe and harmful. If we had a magic wand we would make them go away. The reality is, however, that we live in a world with many pathogens and have lived in a symbiotic relationship with them for millennia. Our collective goals should be to balance all cause harms and prevent severe outcomes to the extent that medical science provides.
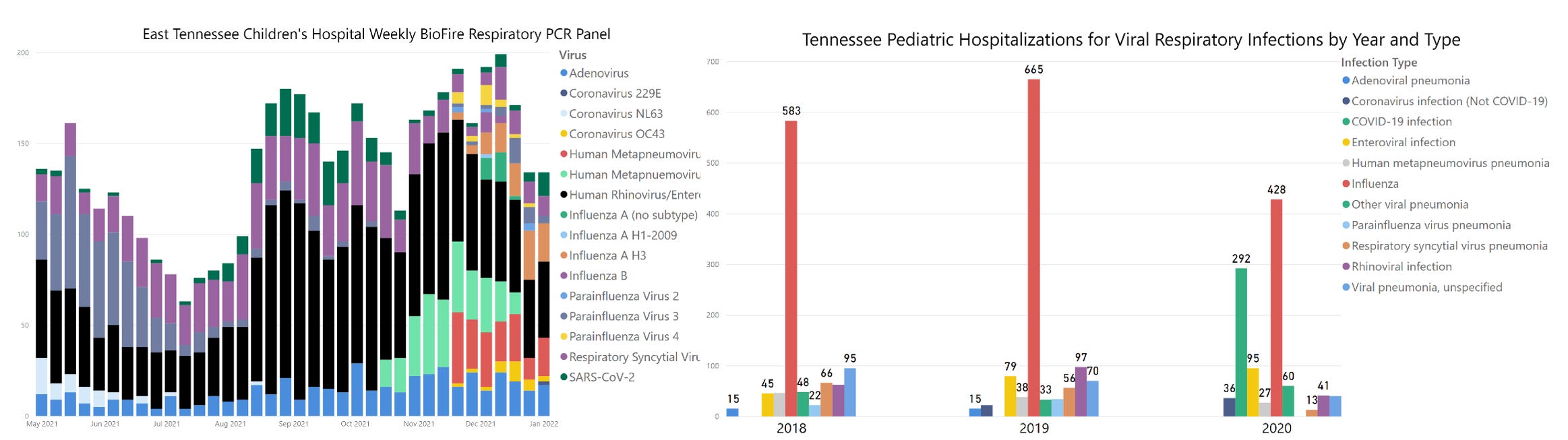
Here’s a static preview of the interactive dashboard below. I have pulled together respiratory virus PCR data from a Children’s hospital in East Tennessee, and a report on annual pediatric hospital admissions for respiratory disease from the Tennessee Department of Health. I hope this might help to put SARS-COV2 detections in children into perspective.
Paid subscribers can click below to interact with the data.
Keep reading with a 7-day free trial
Subscribe to Relevant Data to keep reading this post and get 7 days of free access to the full post archives.